





- Labor’s share of total hospital expenses has increased in the last 10 years.
- Certain factors are accelerating hospital labor costs, such as a tightening labor market, which drives up wages.
- Successful efforts to control labor costs include strategies to improve retention of clinical staff.
- Hospitals also are saving money by increasing the role of automation in the revenue cycle.
Hospitals have been on a hiring spree since the Great Recession in response to pressures from increasing quality requirements, consumerism, new missions and an aging patient population.
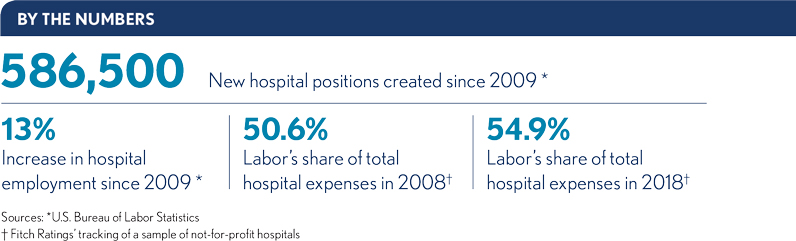
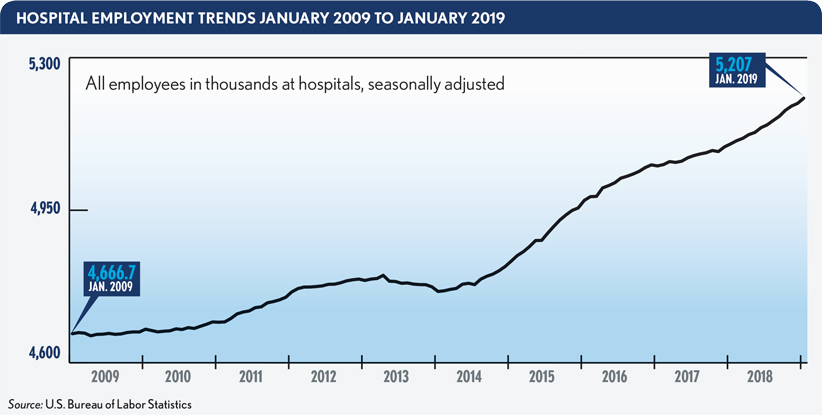
But all those new positions — amounting to 586,500 new hospital jobs over the past 10 years, according to data from the U.S. Bureau of Labor Statistics — have increased cost pressure that finance leaders must contend with. And more of those executives are taking note of labor’s increasing cost burden and the importance of addressing it before public and private health plans slash hospital payment rates.
“The overall expense of labor is increasing, but more hospital leaders also are focused on labor,” says Erik Swanson, a vice president at the Skokie, Illinois-based consultancy Kaufman, Hall & Associates, LLC.
See related sidebar: Control labor costs with a 7-pronged approach
An example of that burden was that labor’s share of total expenses increased steadily from 2008 to 2018, rising from 50.6% to 54.9% among hospitals tracked by Fitch Ratings.
Although hospitals’ labor costs are manageable when they hover around 50%, organizations’ financial positions worsen as the costs rise much above that, says Robin Czajka, a vice president for Premier Inc., a hospital advisory alliance based in Charlotte, North Carolina. (See the sidebar, where Czajka recommends seven steps for controlling labor costs.)
Increasingly unwieldy labor costs will leave hospitals vulnerable as some policymakers push for broader adoption of Medicare rates and as private health plans continue to cut provider prices, says Michael Chernew, PhD, a professor of healthcare policy at Harvard Medical School. Those cuts will force hospitals to figure out how to operate with less revenue while still providing high-quality care.
“We know it’s possible, because broadly speaking it seems like some facilities can do that. But we don’t know, I don’t know, exactly what the right recommendation would be for any particular hospital,” Chernew says.
What’s driving labor cost increases?
The largest segments of the newly added positions reflected the already-largest groups of hospital workers, including nurses, technicians, physicians and physician assistants, says Ani Turner, a co-director of Sustainable Health Spending Strategies, with a focus on health employment, at Ann Arbor, Michigan-based Altarum.
Added to those growing numbers of traditional hospital employees were new types of staff needed to fulfill missions hospitals took on in the past decade, including implementation of electronic health records (EHRs) and other IT initiatives, population health management, cross-provider care coordination, tracking of social determinants of health and development of innovation hubs, says Kevin Holloran, senior director and sector leader of the Not-for-Profit Healthcare Group in Fitch Ratings’ public finance department.
These days, Holloran says, labor is always among the top three costs hospital CFOs want to discuss with him.
Other factors that drove labor cost increases over the past 10 years, according to Holloran, include:
- A tightening labor market and the higher wages it demands
- Aging patients with increasingly acute conditions
- The growing population
- Increasing patient access points through more physician practices, urgent care centers and ambulatory surgical centers
- Healthcare organizations’ responses to consumerism
The consumerism focus, for example, has led hospitals to add staff as navigators to guide patients requiring surgery through the system and as concierge staff to answer nonclinical questions, such as requests for the hospital’s Wi-Fi password, Holloran says. Such new positions aim to improve patient experience with the organization and preference to receive future treatment from that provider.
“You go back 10 years, 20 years, it’s all about us — it’s all about the doctors and the hospitals, and we just do it our way because it works for us,” Holloran says. “We’ve shifted the paradigm to ‘What works for you?’ and ‘Let’s get you there.’ A lot of that is more bodies and more people just trying to help us deal with the complexities of the experience.”
Connections and educational offerings help retention
Nurses constitute half of hospitals’ clinical workforces, says Therese Fitzpatrick, PhD, RN, a senior vice president for Kaufman Hall and a former hospital CNO.
“There are organizations using traditional staffing approaches and not getting the results they got in the past,” Fitzpatrick says about organizations where nurse staffing is determined through a three-day census and application of a productivity factor adjustment (such as a relative-value unit). “That staffing model lacks promise.”
A common result of such approaches is dissatisfaction among nurses over a deviation from what they view as promised staffing levels, leading to their eventual departure from the organization. High turnover rates are an increasing problem, and cost driver, in a tight labor market.
Northwell Health, located in the high-cost New York market where labor costs have increased in recent years to reach 63% of total operating expenses, saw costs increase after 2010, when it implemented a requirement that its nurses have, at a minimum, bachelor’s degrees. Since then, it launched a growing number of initiatives aimed at improving retention of nurses and other high-cost staff, says Joseph Moscola, senior vice president and chief people officer for Northwell Health.

In addition to the CEO’s high-profile, weekly two-hour meeting with, on average, as many as 175 new hires and transferring employees at the 70,000-employee health system, the organization is focused on nontraditional ways to make connections with employees. Moscola believes one of the reasons people stay in an organization is the relationships they develop there. “So to the extent that we can create comradery, we do that, as well,” he says.
Other efforts to improve retention included adding ways for Northwell employees to advance their careers. An example was the launch of a school for nurses and physician assistants in partnership with Hofstra University that includes a track for nurse practitioners.
The efforts were credited with reducing the organization’s turnover rate to 9% and allowing average tenure to reach 9.5 years.
Czajka says the retention challenge is a common clinical-labor cost driver for hospitals.
“They haven’t figured out the secret sauce to keeping nurses and lab workers and pharmacists and ancillary staff,” Czajka says. “So they lose people and end up having to engage premium labor.”
The response of not-for-profit Northwell to the costly contract-worker challenge was for its human resources department to launch a for-profit temp worker and travel nurse agency, called FlexStaff. That entity has allowed the health system to cut its temporary staff costs by focusing on converting temps to permanent employees and avoiding agency service charges. Through also eliminating premium travel agency payments, the subsidiary overall was credited with saving Northwell $38 million over four years, Moscola says.
Automated revenue cycle savings
Scott Johnson, FHFMA, MBA, executive vice president and CFO of St. Luke’s Health Corp., a two-hospital health system based in St. Louis has found automation can provide labor savings within the revenue cycle function.
“It’s a great way for us to consider automating some processes that are fairly redundant and high volume in the revenue cycle,” Johnson said about efforts related to prior-authorization compliance and payment denial research. “There’s all kinds of busywork being done by people that is tedious, and it became clear that to some extent those are basic rule-based functions you could automate with an RPA [robotic process automation] tool.”
One RPA system St. Luke’s has added replaced staff manually logging into the health plans’ websites to confirm that each claim was adjudicated properly.
“Instead, you have a computer do that, constantly pinging the payer database for an immediate answer,” Johnson said.
Johnson says many hospitals already own IT systems that include RPA-type assistance for repetitive tasks but don’t realize it. For instance, a module was available within the health system’s HR payroll system to allow managers to automate tedious tasks of posting job notices, reviewing basic qualifications of applicants and moving the application through the various approvals required from staff on multiple levels.
“Sometimes you just need to get inside your own systems and say ‘OK, is this system capable of performing more for us and have we explored that first?’” Johnson says.
Kelley Blair, a senior vice president for Change Healthcare in Chicago, says other labor savings in revenue cycle operations that hospitals have achieved in recent years have come from:
- Increasing use of work-from-home administrative positions
- Leveraging global talent
- Shifting revenue cycle staff replaced by AI to the task of auditing the AI’s claim work
The shift to overseas financial office contractors, which can cut labor costs in half, has moved beyond accounts receivable management, Blair says, and healthcare organizations are increasingly willing to look at patient interaction functions, such as business office call centers and patient scheduling.
Blair said such outsourcing is difficult for hospitals because such moves raise concerns the community-based organizations are taking jobs out of the community. Overseas contracting also can detract from hospitals’ ability to ensure patients have an excellent experience that will strengthen their loyalty to the health system, which is hugely important in the era of consumerism. However, health plans have long adopted this strategy, and physician groups are increasingly doing so too.
Additional labor savings can be provided by increased use of analytics to change workflows in the revenue cycle. That can allow hospitals to switch from labor-intensive monthly reporting or root-cause analysis in response to health plan payment denials to real-time tracking of claims. Use of analytics allows hospitals to identify all pending transactions similar to rejected claims and to address them all simultaneously to prevent denials, Blair says.
Focusing on a stealth cost
Gerard Brogan Jr., MD, senior vice president and chief revenue officer of Northwell Health, says he has found high turnover is a revenue cycle labor “stealth cost,” as new hires take time to find, train and get up to the speed of existing employees. In response, the health system has implemented leadership training and career development to minimize turnover and to encourage employees who want new jobs to move within the organization instead of leaving.
Among the available labor-savings initiatives, Brogan warns hospital leaders to use caution when bringing in external contractors to implement process changes. “There is an assumption as to the efficiency and effectiveness of that process change, and it may not be monitored as closely as it needs to be,” Brogan says. “And it may not actually have resulted in any improved outcomes, versus what could have been done internally.”

Hospitals also need to spend the time to carefully ensure that potential labor- saving technology interfaces with various software systems they have and that they can effectively review its functionality.
“We’ve had a couple instances where we had significant delays and cost overruns because something that supposedly could interface with a host system really never had been built to do that,” Brogan says. “It was a lesson learned that cost us time and money.”
Outlook: Labor costs will continue rising
The increasing array of hospital responses to labor costs likely will continue to expand, as the workforce shifts from one dominated by baby boomers to one dominated by millennials, industry advisers suggest. And looming health plan payment trends could accelerate the continuing need for labor savings and implementation of such initiatives well into the future.